



Intermittent Facial Flushing and Diarrhea
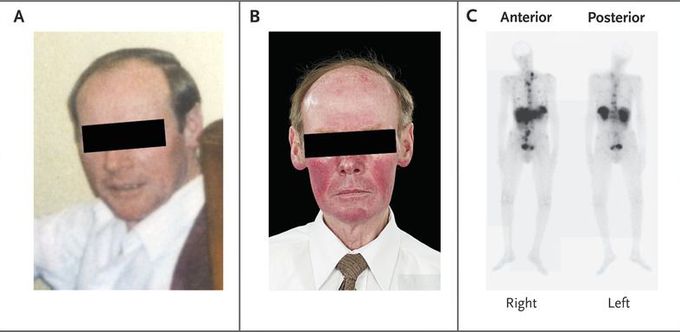
A 67-year-old man presented to his general practitioner with a history of vague abdominal discomfort on the right side, intermittent diarrhea, and episodes of facial flushing every 2 to 3 days. He reported no history of ingestion of alcohol or other precipitants of flushing. Images obtained before and after the onset of symptoms show the patient without and with a flush (Panels A and B, respectively). Two hepatic lesions were detected on ultrasonography, and an additional hepatic lesion and a mass in the midgut were seen on computed tomography (CT). An ultrasound-guided liver biopsy was performed, and histologic analysis of the biopsy specimen revealed a well-differentiated neuroendocrine tumor. The chromogranin A level was elevated, at 765 ng per milliliter (normal range, 19.4 to 98.1), and a 24-hour urinary collection showed a 5-hydroxyindoleacetic acid level of 1524 μmol (normal range, 2.5 to 50.0 μmol). Scintigraphy performed with the use of indium-111–labeled pentetreotide revealed metastases in the liver and the axial skeleton (Panel C). The patient was treated with octreotide; the diarrhea ceased, and the frequency of facial flushing was reduced. However, a CT scan obtained at a 2-year follow-up showed progressive liver and bone metastases, and the treatment was changed to everolimus, which was followed by clinical and radiologic improvement. A recent echocardiogram showed trace tricuspid regurgitation.

I was diagnosed as a Hepatitis B carrier in 2015, with early signs of liver fibrosis. At first, antiviral medications helped control the virus but over time, resistance developed, and the effectiveness faded. I began to lose hope. In 2021, I discovered NaturePath Herbal Clinic despite my skepticism, I decided to give their herbal treatment a try.To my surprise, after just six months, my blood tests came back negative for the virus.It was nothing short of life-changing.I never expected such incredible results from a natural treatment. But it not only cleared the virus it restored my hope, my health, and my peace of mind.If you or someone you know is battling Hepatitis B, I truly encourage you to explore the natural healing path offered by NaturePath Herbal Clinic. It gave me a second chance and it might do the same for you.www.naturepathherbalclinic.com info@naturepathherbalclinic.com
