



DR MOHAMMED IRFAN SHEIKH about 1 year ago
Mechanical Small-Bowel Obstruction
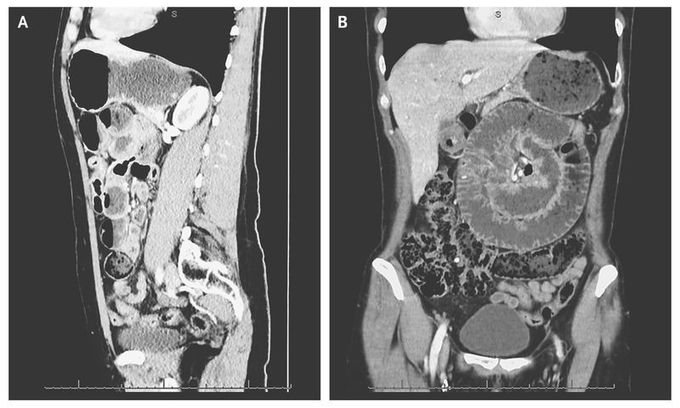
A 57-year-old woman was admitted to the emergency department with sudden-onset upper abdominal pain and vomiting. The patient's medical history was notable for type 1 diabetes and laparoscopic tubal sterilization. Computed tomography (CT) revealed small-bowel volvulus with dilated small bowel rotated around its blood supply (Panels A and B). There were no signs of free air or fluid and no indication of bowel ischemia on the CT scan. Explorative laparotomy revealed signs of strangulation of the small bowel 1 m from the ligament of Treitz. The bowel was viable, and no resection was performed. The patient was discharged in good condition 3 days later.
Other commentsSign in to post comments. You don't have an account? Sign up now!
