



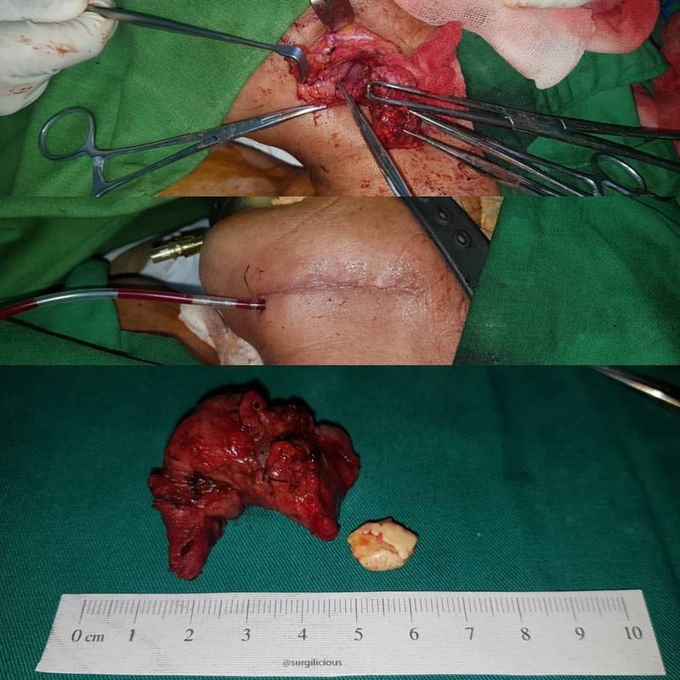
Sialolithiasis
Sialolithiasis should be considered in the differential diagnosis of any patient with chronic or recurrent salivary gland swelling or inflammation. It occurs most frequently in Wharton’s duct followed by Stenson’s duct, and rarely in the sublingual glands. In the acute setting, patients with sialadenitis secondary to calculi are treated conservatively with antibiotics, and stones less than 2mm may pass spontaneously. Stone formation is more frequent in areas where the duct is narrow or compressed. Management of sialoliths depends on the stone size, location, number of stones and the extent of ductal obstruction. Surgical management ranges from minimally invasive to open surgical techniques Sialoliths are composed of both organic and inorganic substances. They are thought to originate from secretory inactivity of the salivary gland leading to creation and accumulation of sialomicroliths. These in turn become colonized with bacteria leading to duct inflammation with cellular exudate and fibrosis. Risk factors include dehydration, certain medications such as diuretics, anticholinergics, and antihistamines, certain autoimmune conditions, systematic abnormalities with calcium metabolism, and altered salivary pH. The submandibular gland is more frequently excised for chronic sialadenitis secondary to lithiasis. Risks include marginal mandibular nerve weakness.
