



Aortic Dissection
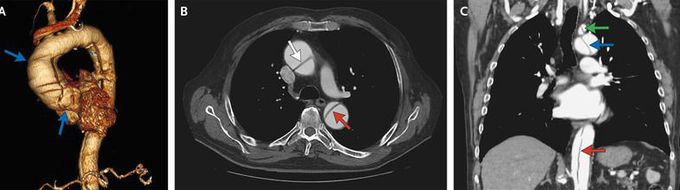
An 81-year-old man with no documented medical history presented to the emergency department with suprapubic pain and urinary retention resulting from benign prostatic hyperplasia. He was incidentally found to have an elevated troponin I level, at 0.17 ng per milliliter (normal value, <0.08). He reported no chest or back pain or shortness of breath. There was no evidence of ischemic changes on electrocardiography. Chest radiography showed widening of the mediastinum. Transthoracic echocardiography showed aneurysmal dilatation and a dissection flap in the ascending aorta (video). Computed tomographic angiography of the thorax and abdomen revealed an ascending aortic aneurysm (Panel A, blue arrows) and a type I DeBakey aortic dissection. The dissection involved the ascending aorta (Panel B, white arrow), aortic arch (Panel C, blue arrow), and descending aorta (Panels B and C, red arrows), terminating just below the origin of the renal arteries. Several branch vessels were involved as well, including the right brachiocephalic artery, left subclavian artery (Panel C, green arrow), and superior mesenteric artery. Given the absence of associated symptoms, the dissection was thought to be chronic. The patient declined consideration of surgical intervention but agreed to treatment with a beta-blocker. One year later, the patient's condition had not worsened; he continued to be treated with a beta-blocker and to receive routine follow-up care.
Video link. https://youtu.be/f_Np9xsPztY
