



Enteroenteric Intussusception
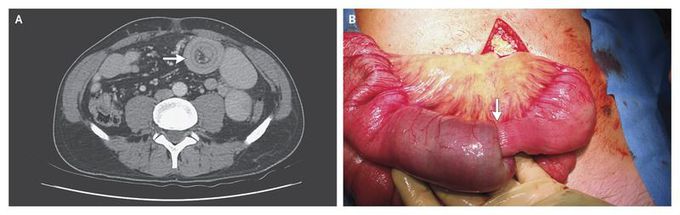
A previously healthy 52-year-old man with epigastric pain and nausea was transferred to our hospital after computed tomography (CT) of the abdomen revealed findings suggestive of enteroenteric intussusception. He was treated successfully with conservative therapy. Three days after his discharge, while awaiting the results of further diagnostic studies, he presented with similar symptoms. On physical examination, he appeared to be moderately ill, with diffuse abdominal discomfort; there were no clinical signs of peritonitis. All laboratory tests were unrevealing. CT of the abdomen, which was performed on readmission, showed dilated small-bowel loops and a “target sign” (Panel A, arrow), findings characteristic of intussusception, without evidence of a lead point. A laparotomy was performed, and the findings confirmed the suspected diagnosis of jejunojejunal intussusception. There was ischemic discoloration of the small bowel, and an intraluminal tumor was felt at the lead point of the intussusception (Panel B, arrow). A 15-cm segment of the proximal jejunum was resected, and a side-to-side anastomosis was performed. Pathological examination of the specimen revealed a 5.5-cm T2N0 adenocarcinoma, with clear resection margins. The postoperative course was unremarkable, and the patient was doing well at an 8-month follow-up visit.
