



African Tick-Bite Fever after a Game-Hunting Expedition
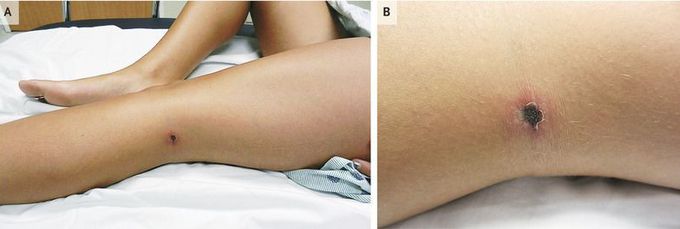
A 15-year-old girl was admitted to the hospital with a 2-week history of persistent fever, headache, and myalgia. A solitary, painful, black, crusted ulcer with a peripheral erythematous halo was noted in the left popliteal fossa (Panels A and B); the ulcer had begun as an asymptomatic erythematous papule 1 week earlier. Associated inguinal lymphadenopathy was also present. The patient, who reported handling a tick-infested antelope carcass and hiking through the brush in shorts during a recent hunting trip to South Africa, had returned to Texas 10 days before hospital admission. Initial serologic testing for rickettsial species was negative. Two punch-biopsy specimens of the eschar were taken concurrently for histopathological testing and special studies. Histopathological testing of the first specimen revealed a small-vessel vasculitis with extensive mononuclear inflammatory-cell infiltrate and scattered neutrophilsorganisms were identified. The second biopsy specimen was sent to the Centers for Disease Control and Prevention, where polymerase-chain-reaction testing was positive for Rickettsia africae. R. africae is an intracellular bacterium that causes the zoonosis African tick-bite fever, which is characterized by fever, myalgia, headache, regional lymphadenitis, and one or more inoculation eschars. R. africae has been isolated from tick vectors of the amblyomma genus or from infected humans in more than 15 African countries and appears to be an emerging cause of influenza-like illness in travelers. The patient began taking doxycycline and was discharged 3 days after admission. No other members of her hunting party reported illness. The patient has done well after discharge from the hospital and is without any known sequelae.
