



Calcinosis in Juvenile Dermatomyositis
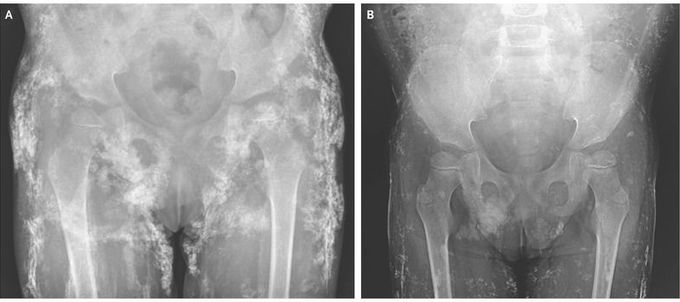
A 4-year-old girl with juvenile dermatomyositis was brought to the rheumatology clinic with a rash and limb weakness. She had had continuous disease activity without remission despite receiving treatment with multiple medications, including glucocorticoids, intravenous immune globulin, methotrexate, and cyclosporine, over a period of 3 years at another hospital. On physical examination, the patient had erythematous changes to the skin overlying the finger, knee, and elbow joints (findings consistent with Gottron’s sign), heliotrope rash around the eyes, proximal muscle weakness in the arms and legs, and diffuse, palpable subcutaneous nodules. A radiograph of the pelvis showed extensive calcification (Panel A). Magnetic resonance imaging of the thighs revealed muscle inflammation and calcinosis. The results of laboratory testing showed strong anti–nuclear matrix protein 2 (anti–NXP-2) autoantibody positivity, a finding associated with calcinosis in juvenile dermatomyositis. Given the patient’s refractory juvenile dermatomyositis and severe calcinosis, treatment with infliximab, thalidomide, and aluminum hydroxide was initiated. Two months after treatment, the patient had improved muscle strength and fading of the rash. At 9 months of treatment, a repeat radiograph showed that the calcinosis had decreased (Panel B).
Thank you! This is the kind of content I want from this app!
