



Trapped Lung
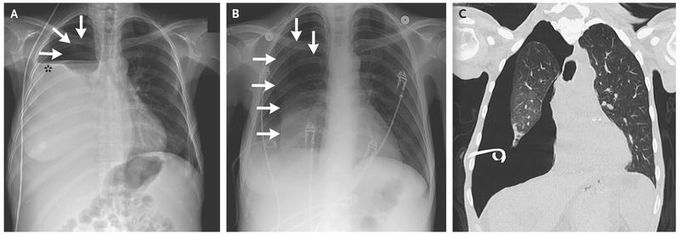
A 46-year-old woman with end-stage liver disease that was complicated by recurrent hepatic hydrothorax requiring multiple thoracenteses presented with breathlessness. Chest examination found no breath sounds on the right side. Radiography of the chest revealed a hydropneumothorax (Panel A; the arrows indicate pneumothorax, and the asterisk hydrothorax). The hydrothorax was drained with the use of a pigtail catheter, with persistent pneumothorax (Panel B, arrows). A computed tomographic scan of the chest showed trapped lung (pneumothorax ex vacuo) with thickened visceral pleura and no evidence of endobronchial obstruction (Panel C). Trapped lung is due to fibrous visceral pleural thickening from a chronic inflammatory process that prevents lung reexpansion. The noncompliant lung separates from the parietal pleura, and this space fills with fluid, with resultant hydropneumothorax. Drainage of the pleural fluid leads to pneumothorax ex vacuo because the lung cannot reexpand to fill the chest cavity. Once other causes of pneumothorax ex vacuo, such as endobronchial obstruction, are excluded, the management of trapped lung is surgical, with removal of the fibrosed visceral pleura to allow for the expansion of the underlying lung. In this patient, video-assisted thoracoscopic surgery with decortication and pleurodesis was performed, with complete reexpansion of the right lung.

I was diagnosed as a Hepatitis B carrier in 2015, with early signs of liver fibrosis. At first, antiviral medications helped control the virus but over time, resistance developed, and the effectiveness faded. I began to lose hope. In 2021, I discovered NaturePath Herbal Clinic despite my skepticism, I decided to give their herbal treatment a try.To my surprise, after just six months, my blood tests came back negative for the virus.It was nothing short of life-changing.I never expected such incredible results from a natural treatment. But it not only cleared the virus it restored my hope, my health, and my peace of mind.If you or someone you know is battling Hepatitis B, I truly encourage you to explore the natural healing path offered by NaturePath Herbal Clinic. It gave me a second chance and it might do the same for you.www.naturepathherbalclinic.com info@naturepathherbalclinic.com
