



Measles
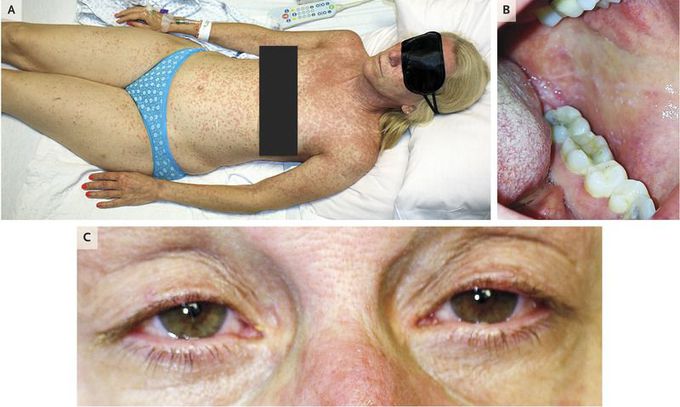
A 54-year-old woman presented with 5 days of fever, cough, and rhinorrhea after returning to the United States from a missionary visit to the Philippines. She had no clinically significant medical history and did not recall having had measles. She reported full vaccination as a child, including the measles vaccine, although records of dosing and strain were not available. Examination revealed an exanthem involving the head, neck, and shoulders with cephalocaudal spread (Panel A), small white papules on buccal mucosa bilaterally (Panel B), conjunctivitis with serous discharge (Panel C), and cervical lymphadenopathy. Laboratory evaluation showed elevated aminotransferase levels, leukopenia, and thrombocytopenia. The patient was placed in an airborne-infection isolation room immediately on suspicion of measles. Serologic testing revealed elevated antirubeola IgM titers (4.4 times the upper limit of the normal range) and negative antirubeola IgG titers. This case highlights classic clinical features of measles, the need for clinical suspicion in travelers returning from high-risk areas, and the risk of inadequate immunity, even among immunized persons. The patient received supportive care, including vitamin A supplementation, for a diagnosis of measles, from which she had a full recovery.
Measles cause by viral infection, self limiting diseases. Need bed rest, good nutrition and symphtomatic drug.
