



Subglottic Stenosis
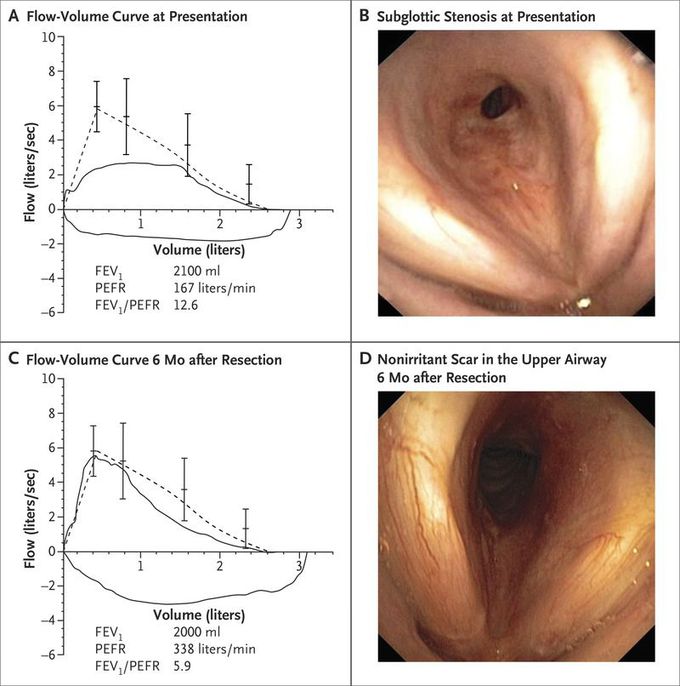
A 55-year-old woman presented with a 6-month history of exercise-induced dyspnea and intermittent wheezing. Clinical examination revealed inspiratory stridor. Spirometry revealed a flattened inspiratory and expiratory flow-volume loop (Panel A; the dotted line indicates the reference curve, and the vertical lines means with 95% confidence intervals) and an Empey index (the forced expiratory volume in 1 second [FEV1] in milliliters divided by the peak expiratory flow rate [PEFR] in liters per minute) of 12.6, suggesting upper-airway obstruction. Bronchoscopy revealed subglottic stenosis (Panel B). Computed tomography revealed a concentric stenotic tracheal segment without external compression. Cricotracheal resection with end-to-end anastomosis was performed. Histopathological analysis revealed chronic fibrosing inflammation without evidence of cancer, vasculitis, or granulomas. A diagnosis of idiopathic subglottic stenosis was made. A rare inflammatory process of unknown origin, idiopathic subglottic stenosis typically occurs in women and is limited to the subglottic region and the first two tracheal rings. Therapy options include endoscopic procedures, glucocorticoid injections, and resection. Flattened inspiratory and expiratory flow-volume loops on spirometry and an Empey index of more than 10.0 support a diagnosis of fixed upper-airway stenosis. Lung-function testing in this patient 6 months after surgical resection showed near-normalization of the flow-volume Bronchoscopy revealed a nonirritant scar (Panel D).
