



Secondary Palatal Myoclonus
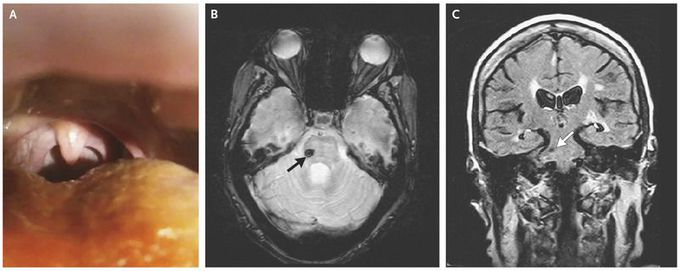
A 59-year-old woman with a history of diabetes, hypertension, and multiple previous strokes presented for evaluation. Two years earlier, she had an acute onset of imbalance, along with difficulty swallowing and speaking. The neurologic examination revealed dysarthric speech and pseudobulbar affect, with a constant, rhythmic jerky movement of the soft palate, which was indicative of palatal myoclonus (Panel A, and Video). She reported having no tinnitus or clicking sounds in her ear, which can be associated with this condition. Magnetic resonance imaging of the brain revealed a hypointense lesion in the right lateral pontine tegmentum on axial gradient echo sequence and coronal fluid-attenuated inversion recovery (FLAIR) sequence (Panels B and C, arrows), suggestive of hemorrhagic stroke. Secondary palatal myoclonus often occurs as a result of a lesion in the brain stem or cerebellum within the triangle of Guillain and Mollaret and is characterized by contractions of the levator veli palatini muscle. Common causes include stroke, neurodegeneration, infections, demyelination, and trauma. Patients with no apparent structural lesion are considered to have essential palatal myoclonus, characterized by contraction of tensor veli palatini muscles, often resulting in repetitive audible ear clicking or tinnitus.
