



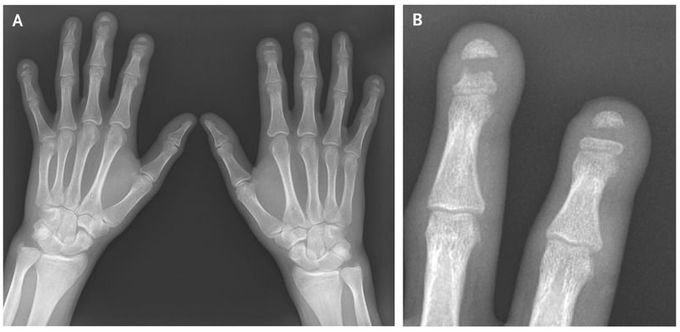
Band Acro-osteolysis
A 23-year-old male construction worker with a history of autoimmune sclerosing cholangitis presented with a 3-year history of coldness affecting both hands, triphasic Raynaud’s phenomenon, and tightening of the skin. Physical examination revealed mild clubbing of the fingers; patchy, nodular thickening of the skin on the hands and forearms; and linear plaques of fibrosis extending proximally past the elbows. His serum was positive for antinuclear antibody (titer, 1:1280) in a homogeneous pattern. Tests for anti–double-stranded DNA, anti-ribonucleoprotein, and anti-Scl-70 antibodies were negative. Plain radiographs of the hands showed sharply demarcated osteolysis of the midshaft of the distal phalanges of the index, middle, and little fingers on both hands and of the left ring finger (Panel A, with Panel B showing an enlarged image of the middle and index fingers of the left hand). This rare finding, known as band acro-osteolysis, has been associated with exposure to polyvinyl chloride (PVC) and with the Hadju–Cheney syndrome. The patient said he had had no exposure to PVC and had no personal or family history of congenital bone dysplasia. Because his symptoms were suggestive of atypical systemic sclerosis, immunosuppressive therapy with mycophenolate was initiated, and treatment with losartan was started for Raynaud’s phenomenon. At 1 year, his condition was clinically and radiologically stable and the Raynaud’s symptoms were reduced.
