



Anterior Thoracic (Chest Wall) Lung Herniation and Repair
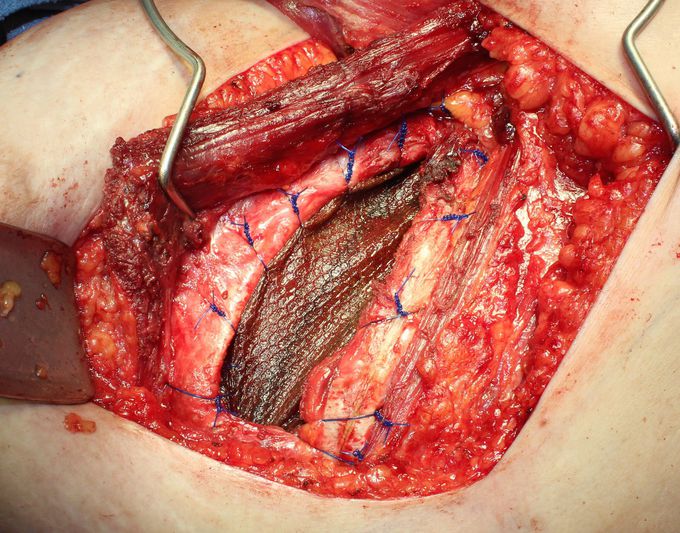
We report a case of acquired anterior thoracic lung herniation in a 63-year-old female. This painful herniation developed four years after uncomplicated video-assisted thoracic surgery for lung cancer resection and adjuvant radiation for concomitant breast cancer. The herniation site was remote from all prior incisions, and demonstrated intercostal muscle denervation and radiation fibrosis. The 8 cm x 10 cm chest wall defect was reconstructed with inlay PROCEED mesh and reinforced with a pedicled latissimus dorsi flap. Six months postoperatively the patient had complete resolution of symptoms, no evidence of herniation, and a stable wound. Lung hernias are subdivided into congenital and acquired cases. Congenital lung hernias account for 18% of cases and involve developmental chest wall defects. Acquired lung hernias can be further classified as traumatic, spontaneous, or pathologic. Traumatic events include surgical procedures and blunt force. Spontaneous lung hernias can be triggered by chronic coughing, COPD, forceful Valsalva, chronic steroid use, or heavy lifting3. Pathological events leading to lung herniation may be inflammatory or neoplastic in nature7. Lung hernias are also classified by location. Seventy percent are thoracic, while the remainder are cervical and diaphragmatic8. The anterior chest wall is inherently prone to lung herniation because only a single layer of intercostal muscle exists parasternally3,9. Lateral and posterior lung herniations are rarely problematic due to the greater support provided by side and back muscles6,10. We believe the lung herniation presented here was likely caused by a combination of events including denervation of muscle in the third intercostal space, resulting from distant VATS, and soft tissue damage from radiation. Fibrosis of muscles after radiation compromises blood supply and innervation, which possibly contributed to the defect. Muscles themselves can also become weakened and easily fatigued following radiation11. There are multiple points during VATS procedures at which injury may occur. The incision may be made with less care, leading to muscle or fascial injury, costal cartilage damage, or muscle denervation. There may also be damage from excessive cauterization or poor dissection2,3. However, this case of lung herniation after uncomplicated VATS demonstrates a chest wall defect that was both temporally and spatially remote from the incision site. The large and worsening defect in this patient required surgical repair. Although smaller defects in the chest wall can be approached with mesh and rib suturing alone, lung hernias due to missing ribs or extensive trauma may require the support and blood supply associated with muscle flaps2. A latissimus dorsi muscle flap was used to reinforce the large inlay mesh repair and provide a reliable source of vascularized tissue to the radiated field. Pedicled muscle flaps are well-tolerated by patients in other procedures. In this case, it resulted in both long-term reduction of the hernia and regaining of strength and range of motion.

What was that...which is inserterd from externally to prevent hernia
