



Metronidazole-Associated Encephalopathy
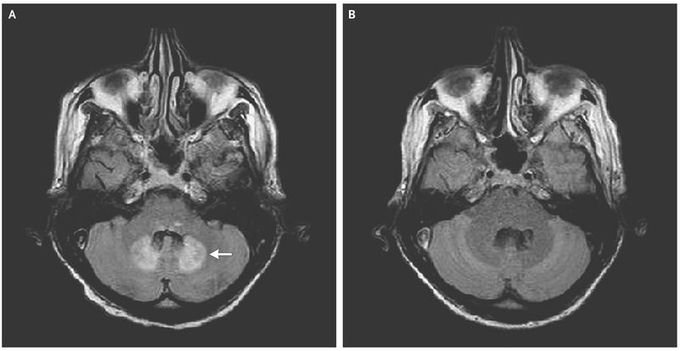
A 58-year-old man with cryptogenic cirrhosis was admitted to the intensive care unit with confusion after a fall at home. He had been taking a prolonged course of metronidazole (500 mg three times per day for >3 weeks) for Clostridium difficile infection. A few days before his hospitalization, dysarthria and gait instability had developed, which had contributed to the fall. A magnetic resonance imaging (MRI) scan of the brain showed a symmetric, enhanced fluid-attenuated inversion recovery (FLAIR) signal in the dentate nuclei of the cerebellum (Panel A, arrow), a finding that is consistent with encephalopathy associated with metronidazole use. On admission, the patient was intubated for airway protection and was sedated; central catheter–related bacteremia developed soon thereafter. Discontinuation of metronidazole resulted in resolution of the imaging findings 1 month later (Panel B). Neurologic assessment was difficult, and the patient never regained his baseline mental status. Encephalopathy associated with metronidazole use is an uncommon side effect of the medication. It typically manifests as dysarthria and gait instability. Risk factors include liver dysfunction and a prolonged course of metronidazole (typical cumulative dose, >20 g). MRI of the brain is usually diagnostic and typically reveals a symmetric, enhanced FLAIR signal in the dentate nuclei of the cerebellum. During the course of hospitalization, this patient died from complications due to central catheter–related bacteremia.
