



Diaphragmatic Hernia Causing Lung Collapse
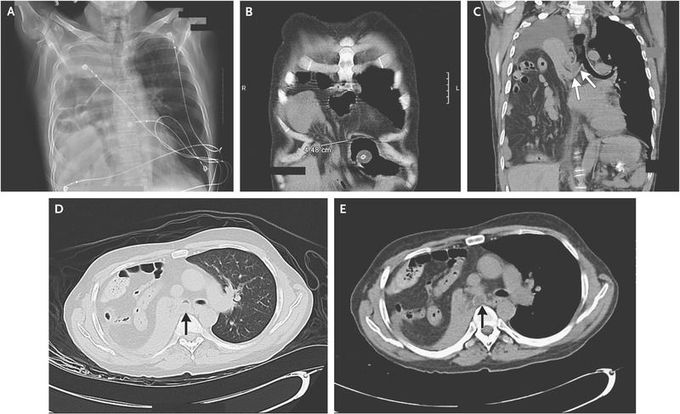
A 54-year-old man with a history of cerebral palsy and mental impairment presented with acute respiratory distress. He was afebrile and had a nonproductive cough. Physical examination revealed the use of accessory muscles of ventilation, decreased right hemithorax expansion, and an absence of breath sounds in the right hemithorax, with audible bowel sounds. The patient had mild hypoxia. A chest radiograph showed near-complete opacification of the right hemithorax, with gas-filled bowel loops on the right that extended to the level of the aortic arch (Panel A). A radiograph obtained approximately 3 months before presentation had shown a small right diaphragmatic hernia. Computed tomography of the chest performed during the current presentation confirmed the presence of a right anteromedial diaphragmatic hernia (Panel B), with a defect in the diaphragm that measured 4.5 cm in diameter. Visible within the right hemithorax was a large volume of abdominal bowel contents (Panels C, D, and E), including the majority of the right colon, the appendix, multiple loops of small bowel, mesenteric fat, and omentum. The right lung was completely collapsed, with mucous plugging of the right mainstem bronchus (arrows). There was only a mild mediastinal shift to the left, a finding that was consistent with the high degree of lung collapse accompanying the hernia and that was probably related to proximal bronchial obstruction. Because of the location of the diaphragmatic defect, the hernia was most likely a Morgagni hernia. These hernias are usually congenital in origin and can increase in size over time, as in this case. In accordance with the wishes of the patient and his family, no surgical repair was attempted.
