



Gastrointestinal Complication of Granulomatosis with Polyangiitis
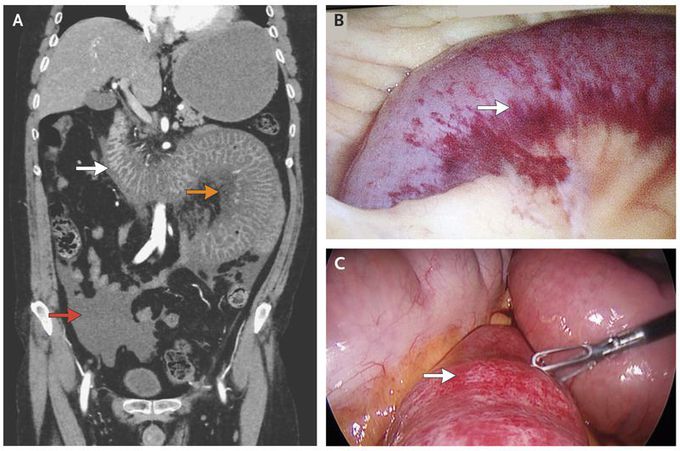
A 48-year-old man who was known to have granulomatosis with polyangiitis was admitted to the hospital for evaluation of an elevated blood creatinine level of 9.5 mg per deciliter (840 μmol per liter; normal range in men, 0.5 to 1.2 mg per deciliter [40 to 110 μmol per liter]). Urinalysis was notable for 2+ protein. The patient, who was positive for antineutrophil cytoplasmic antibody, had been taking azathioprine for 7 years before presentation. Several days after admission, severe abdominal pain developed suddenly, with changes consistent with peritonitis noted on examination. Workup, including computed tomographic angiography, was highly suggestive of bowel ischemia with wall thickening of the distal duodenum and jejunal loops (Panel A, white arrow) with adjacent fat stranding and mesenteric edema (orange arrow) and free fluid in the abdomen and pelvis (red arrow). The patient was taken to the operating room for laparoscopic exploration and was found to have a 40-cm hemorrhagic bowel segment just distal to the ligament of Treitz as well as hemoperitoneum (Panel B shows the involvement of the bowel wall from the mesenteric side and Panel C from the antimesenteric side; the arrow in each panel shows the intraoperative view of hemorrhagic bowel at level of proximal jejunum). The congested hemorrhagic bowel segment was viable, with evidence of active peristalsis, so no bowel resection was performed. This condition was thought to be bowel-wall vasculitis due to granulomatosis with polyangiitis. After surgery, the patient was treated with a heparin drip, and at 48 hours he had minimal abdominal pain. However, he had a persistent elevation of the blood creatinine level. During the same admission, he had rapid progressive worsening of kidney function, and the development of end-stage renal disease necessitated dialysis three times per week. There was no change in his treatment with azathioprine. At a follow-up visit 9 months after presentation, he reported no recurrent abdominal pain, there were no new manifestations of granulomatosis with polyangiitis, and he was receiving permanent renal-replacement therapy.
