



Hyperkalemia after Missed Hemodialysis
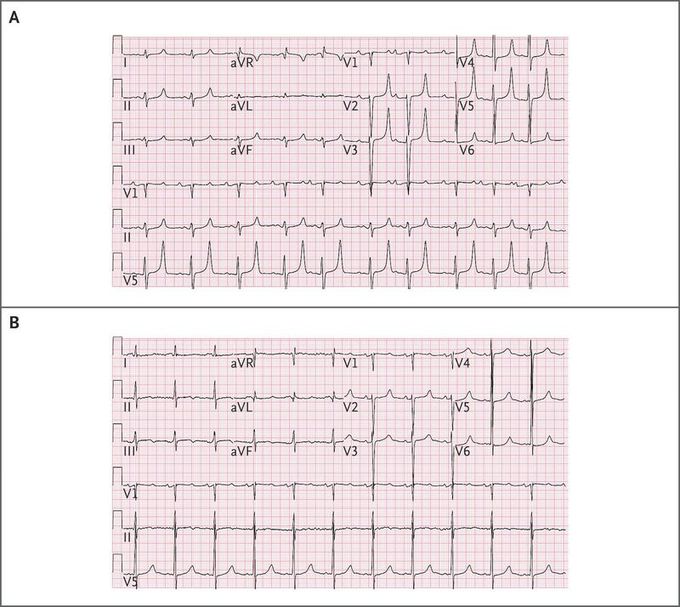
A 48-year-old man with a history of end-stage renal disease who had undergone parathyroidectomy owing to tertiary hyperparathyroidism 1 month earlier presented to the emergency department with weakness and diffuse muscle aches after missing a hemodialysis session. The laboratory analysis showed severe hyperkalemia (potassium level, 36.0 mg per deciliter [9.2 mmol per liter]; normal range, 14.0 to 19.9 mg per deciliter [3.6 to 5.1 mmol per liter]) and severe hypocalcemia (calcium level, 5.0 mg per deciliter [1.25 mmol per liter]; normal range, 8.4 to 10.3 mg per deciliter [2.10 to 2.58 mmol per liter]), with an ionized calcium level of 1.84 mg per deciliter (0.46 mmol per liter; normal range, 4.48 to 5.28 mg per deciliter [1.12 to 1.32 mmol per liter]). The phosphate level was 6.2 mg per deciliter (2.00 mmol per liter), the magnesium level 2.7 mg per deciliter (1.11 mmol per liter), and the albumin level 3.6 g per deciliter. The initial electrocardiogram showed peaked T waves and a prolonged QT segment (Panel A). The patient underwent emergency hemodialysis, which resulted in a marked improvement in the electrolyte balance (potassium level reduced to 17.2 mg per deciliter [4.4 mmol per liter]; calcium level increased to 7.6 mg per deciliter [1.90 mmol per liter]) and the normalization of T waves on the electrocardiogram, although the QT segment remained prolonged (Panel B). The patient’s hospital course was notable for prolonged hypocalcemia, referred to as the “hungry bone syndrome.” It is thought that the acute withdrawal of parathyroid hormone after surgery results in an imbalance of calcium homeostasis, leading to hypocalcemia, hypomagnesemia, hypophosphatemia, and hyperkalemia. After calcium and vitamin D replacement therapy, this patient’s calcium level increased to 7.9 mg per deciliter (1.98 mmol per liter) and the QT segment normalized.
A hyperacute T wave (hyperkalemia) B T wave inversion (hypokalemia and ischemia)
