



Hypopyon and Klebsiella Sepsis
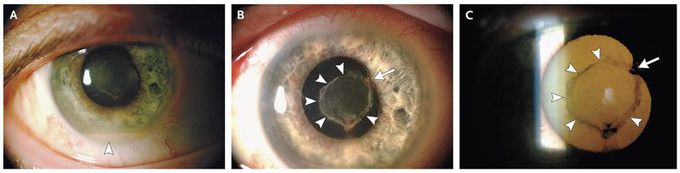
A 49-year-old man with a history of diabetes mellitus reported having blurry vision in the right eye 3 days after being admitted to the hospital for investigation of elevated levels of creatinine, liver enzymes, and bilirubin following 9 days of generalized weakness. He had been receiving treatment for bacteremia caused by Klebsiella pneumoniae associated with bilateral renal cortical abscesses (Fig. S1 in the Supplementary Appendix, The visual acuity of the right eye was “light perception.” The slit-lamp examination showed the presence of hypopyon (a collection of leukocytes in the anterior chamber) (Panel A, arrowhead), posterior synechiae (adhesions of the iris to the lens) (Panels B and C, arrows; broken synechia at 6 o’clock position), and fibrinous exudates covering the anterior lens capsule (Panels B and C, arrowheads). The funduscopic examination revealed dense vitritis. These findings were suggestive of endogenous endophthalmitis. The inflammation resolved but was complicated with vitreous condensation. B-scan ultrasonography (also called brightness scanning) suggested an inferior tractional retinal detachment, for which pars plana vitrectomy with silicone-oil injection was performed. At a 10-week follow-up visit, the patient’s visual acuity in the affected eye had improved to 4/200. K. pneumoniae is a rare but notorious cause of endogenous endophthalmitis, especially among patients of Asian descent with diabetes, and is typically associated with primary liver abscesses. The visual acuity at presentation and early antibiotic treatment are important determinants of disease outcomes.

