



Jejunal Diverticulosis with Midgut Volvulus and Intestinal Malrotation
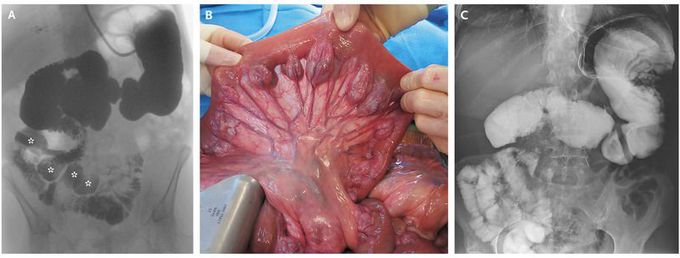
A 67-year-old woman with a 6-month history of malabsorption and malnourishment was referred for possible intestinal transplantation. She had a body-mass index (the weight in kilograms divided by the square of the height in meters) of 19. The patient was receiving only parenteral nutrition because of a long-standing history of jejunal diverticulosis with bacterial overgrowth that was resistant to long-term antibiotic treatment. Six years earlier, a small-bowel derotation and cecopexy had been performed after she had had an episode of gastrointestinal obstruction; however, nausea and diarrhea remained. During the 2 years before the current presentation, she had reported having frequent episodic nausea, abdominal distention, and colic followed by violent fecaloid vomiting. Workup of these symptoms included computed tomography, which showed small-bowel dilatation along with a whirl sign and numerous collateral veins, suggestive of a midgut volvulus (see video). A small-bowel series, performed after decompression by a nasogastric tube, showed the known jejunal diverticulosis (Panel A, asterisks). It also revealed malrotation, with the duodenum not crossing the midline and the jejunum positioned in the right abdomen. Exploratory laparotomy confirmed intestinal malrotation with chronic midgut volvulus, together with a duodenal diverticulum and extensive jejunal mesenteric diverticulosis (Panel B). After resection of the duodenal diverticulum and jejunum and a Ladd procedure, the patient was left with 270 cm of healthy ileum (Panel C). Two months later, the patient had been completely weaned from parenteral nutrition. One year after surgery, her body-mass index had increased to 24, she was symptom-free, and she had returned to a normal lifestyle.
