



Obstructive Hydrocephalus
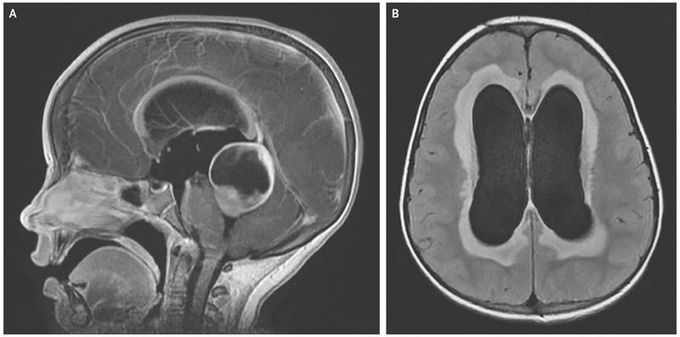
A 4-year-old girl with a 2-week history of progressive headache, nausea, vomiting, and irritability was brought to the emergency department. The patient was confused and combative. She had disconjugate gaze on extraocular examination and also had an unsteady, uncoordinated gait. Contrast-enhanced T1-weighted magnetic resonance imaging revealed a cystic mass measuring 3.4 cm by 3.9 cm by 4.4 cm in the quadrigeminal cistern, arising from the tectal plate and compressing the cerebral aqueduct (Panel A). Its presence resulted in obstructive hydrocephalus and bowing of the corpus callosum. Transependymal flow of the cerebrospinal fluid (CSF) was seen on the axial T2-weighted FLAIR (fluid-attenuated inversion recovery) sequences (Panel B). The patient underwent placement of an external ventricular drain, tumor resection, and endoscopic third ventriculostomy. Histologic examination of the tumor specimen led to a diagnosis of pilocytic astrocytoma. After surgery, the patient had complete resolution of her symptoms, and adjuvant chemotherapy was initiated. At follow-up 9 months after the surgery, the hydrocephalus had resolved without recurrence, and no further diversion of the CSF was required.
