



Takotsubo Cardiomyopathy
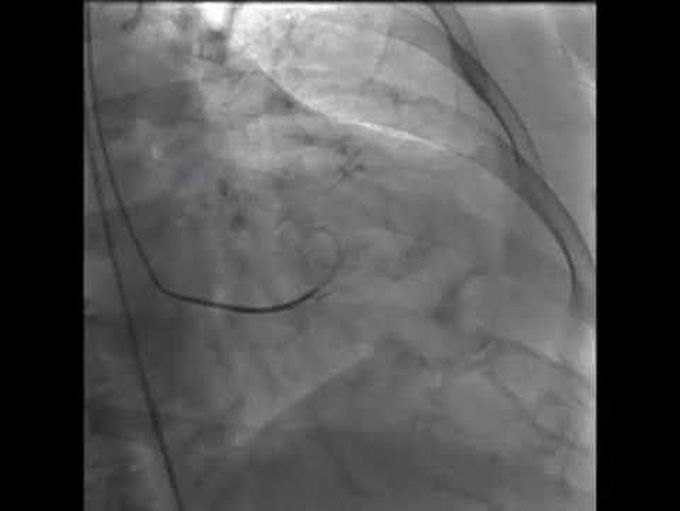
A 61-year-old woman with hypertension and hypothyroidism presented to the emergency department with acute onset of severe chest pain. She reported multiple recent stressors, including the death of her dog. An electrocardiogram showed ST-segment elevation in the anterolateral leads. Emergency coronary angiography revealed normal coronary arteries. Left ventriculography (Video 1 and Panel A [showing diastole] and Panel B [showing systole]) and contrast echocardiography (Video 2) revealed severe hypokinesis in the apical segments and hyperdynamic basal segments, with an ejection fraction of 40 to 45%. A diagnosis of takotsubo cardiomyopathy was made. Takotsubo cardiomyopathy, also called apical ballooning syndrome or stress cardiomyopathy, typically occurs in postmenopausal women and may be preceded by a stressful or emotional event. The clinical presentation may be identical to that seen in patients with acute coronary syndrome, but the condition is characterized by transient left ventricular systolic and diastolic dysfunction of the apex and midventricle in the absence of attributable coronary artery disease. Medical management, including the administration of an angiotensin-converting–enzyme (ACE) inhibitor and a beta-blocker, was initiated, and the patient’s chest pain resolved. An echocardiogram obtained 1 month after presentation showed normalization of cardiac wall motion and an ejection fraction of 65 to 70%. At follow-up 1 year after presentation, the patient remained asymptomatic.
Where does this "takotsubo" term from???........
