



Pigmented Macule — A Skin Manifestation of Invasive Breast Cancer
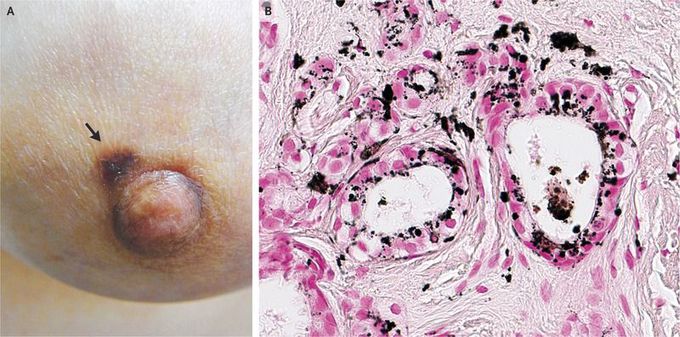
A 62-year-old woman presented to the breast-surgery clinic with stiffness of the left nipple. Palpation of the left breast, mammography, and ultrasonography revealed no abnormalities. However, a pigmented macule that measured 5 mm in the greatest dimension was noted on the left areola (Panel A, arrow). The patient was referred for areolar skin biopsy. Histopathological examination revealed invasive adenocarcinoma in the dermis. On immunohistochemical testing, the cancer cells were strongly positive for estrogen and progesterone receptors and negative for human epidermal growth factor receptor type 2. The glands within the intradermal cancerous lesion were colonized by melanocytes with heavy deposits of melanin granules (Panel B, Fontana–Masson stain). Melanocytic colonization of breast cancers with attendant pigmentation may occur microscopically and can occasionally manifest as skin changes. In this case, the carcinoma arose in the nipple, and conventional breast imaging was not effective for tumor detection. The patient underwent a partial mastectomy, and pathological examination revealed an invasive ductal carcinoma, measuring 9 mm in the greatest dimension, in the nipple. There was no evidence of metastasis. The patient received antiestrogen therapy and underwent radiotherapy. At last follow-up, 10 months after the initiation of treatment, she remains well, with no further symptoms
