



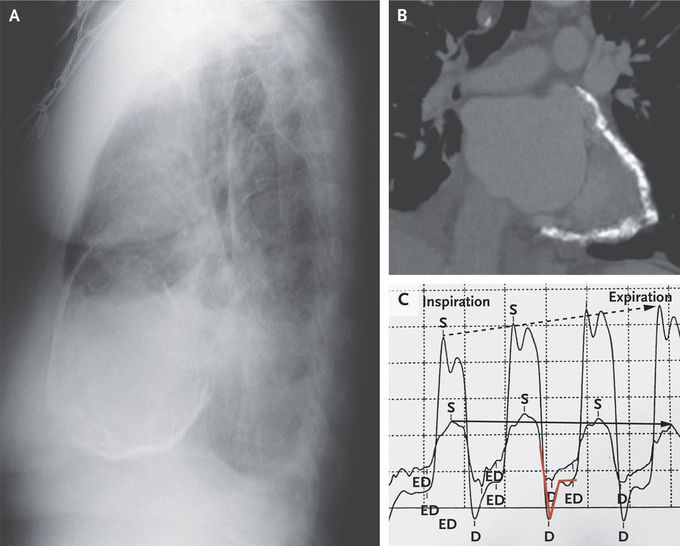
Constrictive Pericarditis
A 69-year-old woman presented to the emergency department with a 3-year history of dyspnea on exertion. She had a history of focal pleural plaques that had been attributed to asbestos exposure that occurred during her work at an insulation-manufacturing company. Physical examination was notable for signs of volume overload. A chest radiograph showed circumferential calcification of the pericardium, pleural effusions, and interstitial edema (Panel A, lateral view). Computed tomography of the chest revealed extensive pericardial calcification (Panel B). A transthoracic echocardiogram showed a preserved ejection fraction with a septal bounce in early diastole as well as expiratory diastolic reversal in the hepatic vein. A subsequent simultaneous left and right heart catheterization showed ventricular interdependence and discordance of the pressure tracings. During inspiration, when pressures in the right ventricle were at their highest, left ventricular pressures were at their lowest; this pattern reversed during expiration (Panel C; right ventricular pressure, solid arrow; left ventricular pressure, dotted arrow). A “square root” sign (also called a dip-and-plateau pattern; Panel C, red line), which represents rapid ventricular filling in early diastole before abrupt cessation in late diastole, was seen. A diagnosis of constrictive pericarditis due to asbestosis was made. A pericardiectomy was performed. Analysis of pericardial tissue was negative for tuberculosis. At 2 years of follow-up, the patient was doing well.

I was diagnosed as a Hepatitis B carrier in 2015, with early signs of liver fibrosis. At first, antiviral medications helped control the virus but over time, resistance developed, and the effectiveness faded. I began to lose hope. In 2021, I discovered NaturePath Herbal Clinic despite my skepticism, I decided to give their herbal treatment a try.To my surprise, after just six months, my blood tests came back negative for the virus.It was nothing short of life-changing.I never expected such incredible results from a natural treatment. But it not only cleared the virus it restored my hope, my health, and my peace of mind.If you or someone you know is battling Hepatitis B, I truly encourage you to explore the natural healing path offered by NaturePath Herbal Clinic. It gave me a second chance and it might do the same for you.www.naturepathherbalclinic.com info@naturepathherbalclinic.com
