



Acrodermatitis Enteropathica
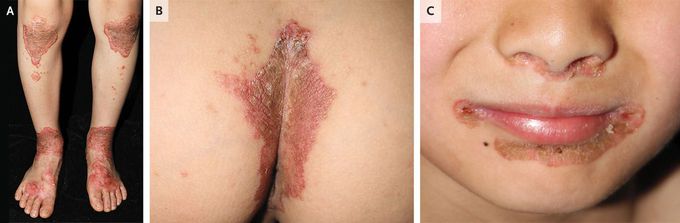
A 9-year-old boy was brought to the pediatric dermatology clinic with a 1-year history of rash and a 3-month history of abdominal pain and diarrhea. At 6 months of age, the patient had begun receiving oral zinc supplementation for zinc deficiency of unknown cause. Since that time, he had continued to receive the same dose without adjustment owing to a lack of access to care during the coronavirus disease 2019 pandemic. On physical examination, his height was below the fifth percentile for age. Erythematous, scaly, clearly demarcated psoriasiform plaques were observed on the knees and dorsal surface of the feet (Panel A), as well as on the gluteal cleft (Panel B) and in inguinal regions. Similar lesions were seen around the mouth and nose (Panel C). The fasting serum zinc level was 386 μg per deciliter (59 μmol per liter) (reference range, 444 to 725 μg per deciliter; 68 to 111 μmol per liter), and the alkaline phosphatase level was low. On genetic testing, a pathogenic variant and a variant of uncertain significance were identified in SLC39A4, a gene that encodes a zinc transporter protein. A diagnosis of acrodermatitis enteropathica — an autosomal recessive disorder of zinc deficiency — was made. The dose of elemental zinc was adjusted for the patient’s body weight, and 2 weeks later, his symptoms had abated. At a 6-month follow-up visit, he was doing well.
