



Japanese Spotted Fever
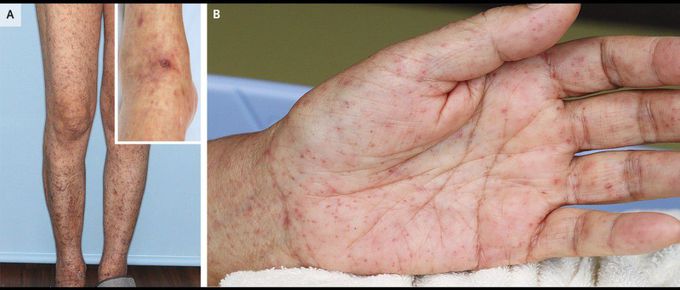
A 68-year-old woman presented to the clinic with a 5-day history of rash, fevers, chills, myalgias, and fatigue. She lived in Japan and had been bitten by a tick on her right ankle 1 week before the onset of symptoms. The rash, which initially had a maculopapular appearance, had erupted abruptly on her arms and legs and had progressed to petechial lesions that also involved the trunk. On examination, the patient’s temperature was 39.2°C. There was a petechial rash on the trunk, arms, legs, palms, and soles (Panels A and B) and an eschar on the right medial ankle (Panel A, inset). She was admitted to the hospital for further evaluation and monitoring. Laboratory studies showed elevated inflammatory markers, a platelet count of 56,000 per cubic millimeter (reference range, 158,000 to 348,000), an alanine aminotransferase level of 98 U per liter (reference range, 10 to 42), and an aspartate aminotransferase level of 165 U per liter (reference range, 13 to 30). Polymerase-chain-reaction testing of a biopsy specimen of the eschar detected Rickettsia japonica. A diagnosis of Japanese spotted fever was made. After the patient completed a 2-week course of minocycline therapy, her symptoms resolved.
