



Fungal Ball in the Urinary Bladder
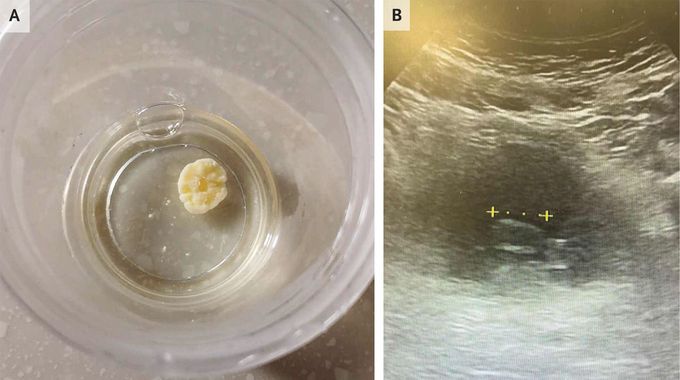
A 68-year-old man with type 2 diabetes presented to the emergency department with a 3-day history of dysuria, intermittent hematuria, and the passage of small balls in his urine with straining. He reported no fever, chills, or flank pain. Three months before presentation, he had started treatment with a sodium–glucose cotransporter 2 (SGLT2) inhibitor. The results of a physical examination were normal. A urine specimen contained a white ball measuring 1.5 cm in diameter (Panel A). Laboratory studies showed a glycated hemoglobin value of 7.8% (reference range, 4 to 6), and a urinalysis revealed glucosuria, pyuria, hematuria, and the presence of yeast. An ultrasound examination showed a 2-cm mobile mass on the bladder floor (Panel B). A urine culture grew Candida albicans, and a diagnosis of candida cystitis with fungal balls was made. Patients with type 2 diabetes are at increased risk for genitourinary infections, and SGLT2 inhibitors may further augment this risk by increasing the degree of glycosuria. This drug class has been more frequently associated with genital mycotic infections, such as candida vaginitis and balanitis, than with fungal urinary tract infections. Treatment with fluconazole was initiated, and the SGLT2 inhibitor therapy was discontinued. Cystoscopy was not performed. At the 4-week follow-up visit, the patient’s symptoms had abated.
