



Radiographic Evolution of Presumed Septic Pulmonary Emboli
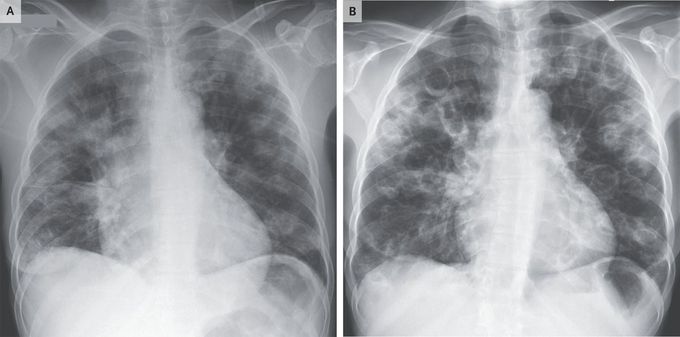
A 41-year-old woman presented to the emergency department with confusion, shortness of breath, and chest pain. She had a history of opioid use disorder and had been injecting drugs daily. Her temperature was 39.4°C, the heart rate was 146 beats per minute, and the oxygen saturation was 80% while the patient was breathing ambient air. On physical examination, she appeared to be ill and had labored respirations, crackles throughout both lungs, and multiple abscesses on her arms and legs. No cardiac murmurs or peripheral stigmata of endocarditis were found. An anteroposterior chest radiograph showed predominantly peripheral, nodular airspace opacities (Panel A). Three sets of blood samples were obtained for culture, and empirical treatment with antimicrobial agents was initiated. Eleven hours later, Gram’s staining identified gram-positive cocci, and rapid polymerase-chain-reaction testing detected methicillin-sensitive Staphylococcus aureus. The patient left the hospital before further diagnostic testing could be completed. She returned 1 week later with worsening of her initial symptoms. A repeat chest radiograph showed progression of the consolidations with interval development of multiple cavitary lesions (Panel B). This finding is suggestive of septic pulmonary emboli in a patient with probable endocarditis on the right side of the heart. Unfortunately, the patient again left the hospital before the completion of further evaluation and treatment, including the performance of echocardiography and referral for therapy for opioid use disorder.
