



Isolated Persistent Left Superior Vena Cava
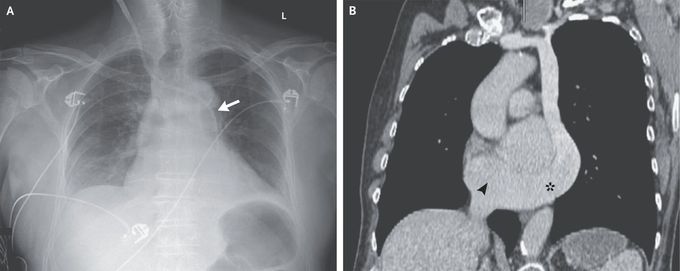
A 79-year-old man with a history of urinary retention that had been treated with an indwelling urinary catheter was admitted to the intensive care unit for septic shock. On hospital day 1, ultrasonographic guidance was used to insert a hemodialysis catheter into the right internal jugular vein to initiate renal replacement therapy for oliguric acute kidney injury. A chest radiograph obtained after the procedure showed the catheter crossing the midline at the level of the manubrium and entering the left mediastinum (Panel A, arrow). Arterial placement of the catheter was initially suspected, although blood gas analysis was consistent with venous placement. Retrospective review of recent computed tomographic images of the chest (Panel B) showed an isolated persistent left superior vena cava coursing along the left mediastinum and subsequently connecting with a large coronary sinus (asterisk) that drained into the right atrium (arrowhead). A persistent left superior vena cava, which is often detected incidentally, is the most common anomaly of the thoracic venous system. It typically occurs simultaneously with a right superior vena cava, which was not found in this patient. Culture of a urine specimen from this patient grew Escherichia coli. After treatment with vasopressors, antibiotic agents, and renal replacement therapy, the septic shock and acute kidney injury resolved. The hemodialysis catheter was removed without complication.
