



Spur-Cell Hemolytic Anemia
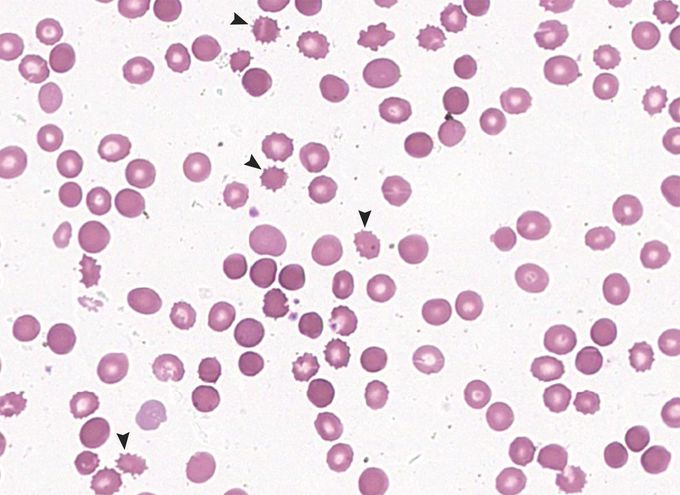
A 48-year-old woman with advanced cirrhosis from alcohol-use disorder presented to the emergency department with a 1-month history of worsening fatigue. On physical examination, she was drowsy and had jaundice and abdominal distention. A digital rectal examination was negative for blood. Laboratory examinations showed a hemoglobin level of 5.8 g per deciliter (reference range, 12.0 to 15.5), a total bilirubin level of 58.4 mg per deciliter (reference range, 0.2 to 1.2), an unconjugated bilirubin level of 26.8 mg per deciliter (reference range, 0.2 to 0.7), a lactate dehydrogenase level of 1219 U per liter (reference range, 125 to 220), a haptoglobin level of less than 8 mg per deciliter (reference range, 14 to 258), and a reticulocyte count of 22% (reference range, 0.5 to 1.8). The result on Coombs’ antiglobulin testing was normal. A peripheral-blood smear showed red cells lacking central pallor with irregularly distributed surface projections, features that are consistent with acanthocytes, or spur cells (arrowheads), which are seen in liver disease, in abetalipoproteinemia, and after splenectomy. These findings led to a diagnosis of spur-cell hemolytic anemia, a type of nonimmune hemolysis that occurs in advanced liver disease owing to excess membrane cholesterol in erythrocytes, a condition that portends a poor prognosis. Because of the severity of her liver disease, the patient was transitioned to hospice care and died at home 2 weeks after discharge.
