



Pediatric Achalasia
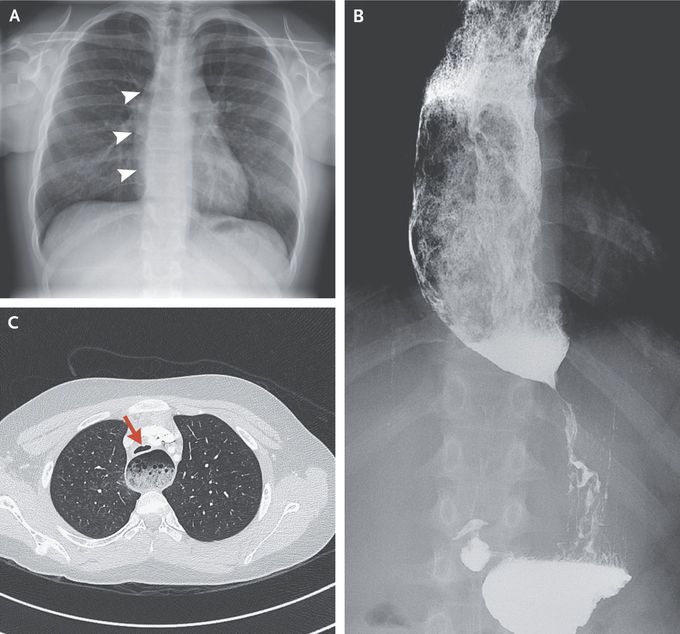
A 13-year-old boy with allergic rhinitis presented to his family physician with a 6-month history of nocturnal cough and nighttime awakenings. The cough had not abated with antibiotic therapy or with medications to treat asthma, gastroesophageal reflux, or postnasal drip. Over the preceding month, he had also begun to have posttussive regurgitation of partially digested food. The physical examination was normal. A radiograph of the chest showed a double contour at the right heart border and widening of the mediastinum, findings that suggested esophageal dilatation (Panel A, arrowheads). A timed esophogram with the use of barium confirmed a dilated esophagus with acute tapering at the gastroesophageal junction (Panel B). Computed tomography of the chest with the use of contrast material revealed a dilated esophagus with intraluminal food and compression and anterior displacement of the trachea (Panel C, arrow). Achalasia may manifest as a nocturnal cough owing to reflux of undigested food during recumbency and is an important consideration in patients whose condition does not improve with therapies for more common disorders. The patient was referred to the gastroenterology clinic and underwent a laparoscopic Heller myotomy with fundoplication. He had no postoperative complications, and his symptoms resolved.
