



Lucio’s Phenomenon
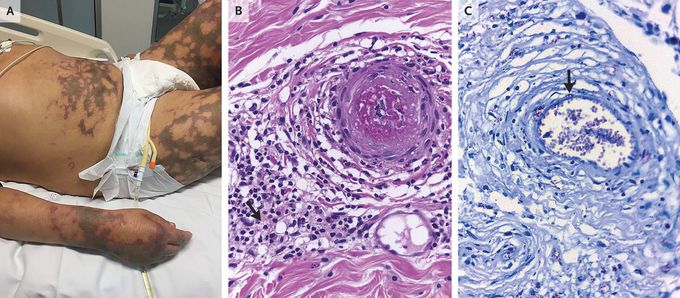
A 48-year-old man presented to the emergency department with a 2-week history of fever, shortness of breath, and painful, blistering skin lesions. His temperature was 39.2°C. Examination revealed retiform purpura and coalescent ulceronecrotic areas over the trunk, arms, and legs (Panel A). Other findings included the loss of both eyebrows, swelling of the earlobes, the absence of wrinkles on the face, and diffuse alopecia. A biopsy specimen of the abdominal skin was obtained, and histopathological analysis revealed thrombosis of medium-sized arteries (Panel B), which were surrounded by a lymphohistiocytic infiltrate that contained plasma cells and foamy macrophages. Fite–Faraco tissue staining revealed multiple acid-fast bacilli, with invasion of the vascular endothelial wall (Panel C, arrow), and a polymerase-chain-reaction assay showed Mycobacterium leprae. The development of severe, necrotizing, cutaneous lesions in patients with diffuse lepromatous leprosy, known as Lucio’s phenomenon, is uncommon. Treatment in this case included multidrug therapy for leprosy (rifampin, clofazimine, and dapsone), systemic glucocorticoids, and anticoagulation therapy. The patient’s fever and dyspnea resolved within 2 weeks after hospital admission, and after several months of wound care, the skin lesions healed, although atrophic and retracted scars remained.
