



Primary Adrenal Lymphoma
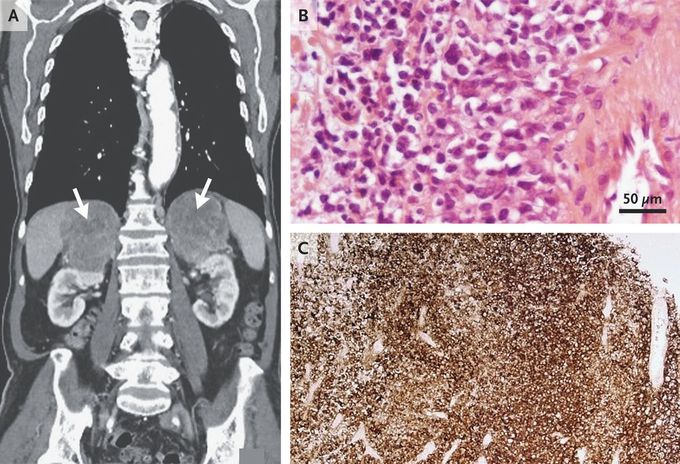
An 83-year-old man with coronary artery disease, hypertension, and hyperlipidemia presented to the emergency department with a 6-week history of fatigue, loss of appetite, and weight loss. His blood pressure was 115/80 mm Hg while he was seated but dropped to 95/65 mm Hg after he stood up. Laboratory studies were notable for a sodium level of 130 mmol per liter (reference range, 133 to 146) and a potassium level of 5.6 mmol per liter (reference range, 3.5 to 5.3). Cosyntropin stimulation testing showed an inadequate peak cortisol level; the corticotropin level was elevated at 87 ng per liter (reference range, 7 to 63). After the patient began treatment with hydrocortisone and fludrocortisone, his energy and appetite improved, and his electrolyte levels normalized. Computed tomography of the abdomen revealed marked enlargement of both adrenal glands, each of which measured more than 9 cm in greatest dimension, without lymphadenopathy (Panel A, arrows). After confirmation of normal plasma metanephrine levels, an adrenal biopsy was performed, which revealed high-grade B-cell lymphoma. Hematoxylin and eosin staining showed nuclear pleomorphism (Panel B), and immunohistochemical staining for the B-cell marker CD20 was positive (Panel C). Primary adrenal lymphoma is rare. It typically occurs in both adrenal glands and may be associated with adrenal insufficiency, as in this case. Chemotherapy was initiated, and the patient was doing well after 3 months.
