



Keratoconjunctivitis Sicca in Sjögren’s Syndrome
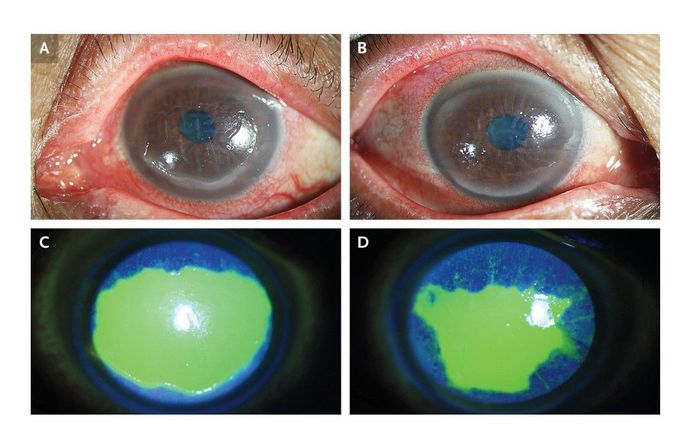
A 64-year-old woman presented to the rheumatology clinic with a 5-month history of photophobia with ocular pain and a foreign-body sensation in both eyes. On further questioning, the patient reported that she had had dry eyes and dry mouth for approximately 20 years without a specific diagnosis or treatment. The visual acuity was 20/25 in each eye, and slit-lamp examination showed conjunctival hyperemia, corneal epithelial erosions, and corneal endothelial folds consistent with keratoconjunctivitis sicca in both eyes (Panels A and B). The corneal lesions were further visualized with fluorescence staining (Panels C and D [green areas]). Schirmer testing showed reduced aqueous tear production, and serologic testing showed an antinuclear antibody titer of 1:160, with antibody positivity for the extractable nuclear Sjögren’s syndrome–related antigen A (Ro52) as well as an elevated rheumatoid factor of 66 IU per milliliter (reference value, <20 IU per milliliter). A diagnosis of Sjögren’s syndrome was made, and treatment for the ocular symptoms included topical cyclosporine A and artificial tears. The symptoms resolved after 2 months.
