



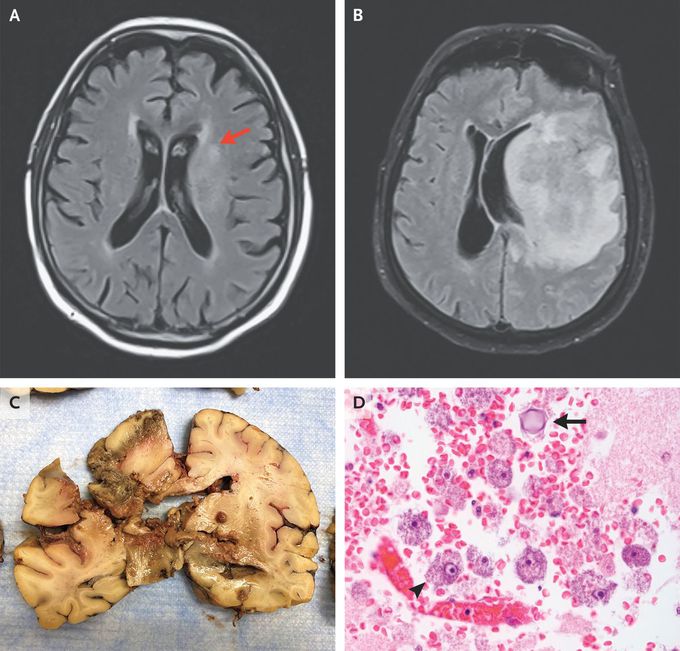
Granulomatous Amebic Encephalitis
An 82-year-old man presented to the emergency department with a 2-week history of generalized weakness. He had a history of B-cell lymphoma that had been in remission for more than 10 years. The physical examination showed diffuse weakness without focal findings. One day after admission, aphasia, weakness on the right side, and altered mental status developed. Magnetic resonance imaging (MRI) showed a nonenhancing signal abnormality in the left paramedian frontal lobe (Panel A, arrow). Analysis of cerebrospinal fluid (CSF) obtained by lumbar puncture showed a protein level of 159 mg per deciliter (reference range, 15 to 45) and 455 nucleated cells, with 22% neutrophils and 46% lymphocytes. CSF cultures were negative, and cytologic analysis showed no malignant cells. Despite receiving treatment for bacterial, fungal, and viral meningitis, the patient became more somnolent and began to have seizures. Repeat MRI 2 days later revealed a large frontal, parietal, and temporal lobe lesion with mass effect (Panel B). The patient died 9 days after presentation. An autopsy showed liquefactive necrosis (Panel C). Trophozoites (arrowhead) and cysts (arrow) were seen by microscopy (Panel D), and polymerase chain reaction identified acanthamoeba species, which confirmed a diagnosis of granulomatous amebic encephalitis. This rare central nervous system infection caused by free-living amebas, particularly acanthamoeba species, is usually fatal. The ameba is transmitted through contact with soil or fresh water. Discussion with the patient’s wife revealed only an exposure to soil from potted-plant maintenance.
