



Naegleria fowleri
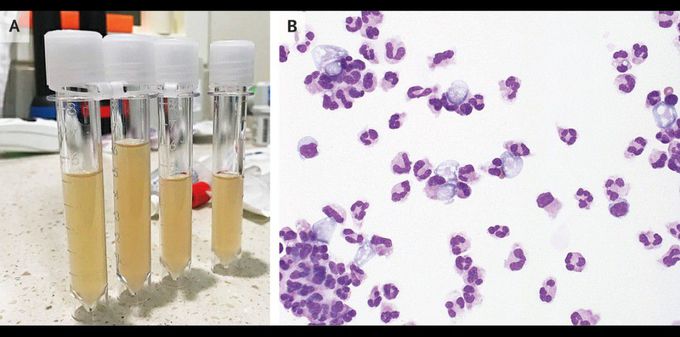
A 44-year-old man presented to the emergency department in January with a 1-day history of confusion and cough. Six days earlier, he had been swimming in an indoor pool in India. At presentation, he had a body temperature of 39.8°C and a heart rate of 120 beats per minute. He did not respond to questions or blink to visual threat; however, brainstem reflexes were intact, and he withdrew both arms and both legs from painful stimuli. He had no nuchal rigidity or rash. A lumbar puncture was performed, and the findings showed purulent fluid (Panel A) with 2083 nucleated cells per cubic millimeter (91% neutrophils), as well as a glucose level of 87 mg per deciliter (4.8 mmol per liter) (reference range, 40 to 70 mg per deciliter [2.2 to 3.9 mmol per liter]) and a protein level of 477 mg per deciliter (reference range, 10 to 45). Empirical antibiotic therapy for bacterial meningitis was initiated; although his fever abated, his mental status did not improve. A review of the wet-mount preparation of the cerebrospinal fluid with the use of a Wright–Giemsa stain revealed trophozoites consistent with amebas (Panel B). A polymerase-chain-reaction assay identified Naegleria fowleri. Usually associated with the summer months and with freshwater, N. fowleri causes primary amebic meningoencephalitis, a disease that is almost universally fatal, although rare cases of survival have been described. Despite treatment that included amphotericin, rifampin, fluconazole, azithromycin, and miltefosine, the patient died 5 days after presentation.
