



Anatomy Of The Infraspinatus Muscle - Everything You Need To Know - Dr. Nabil Ebraheim
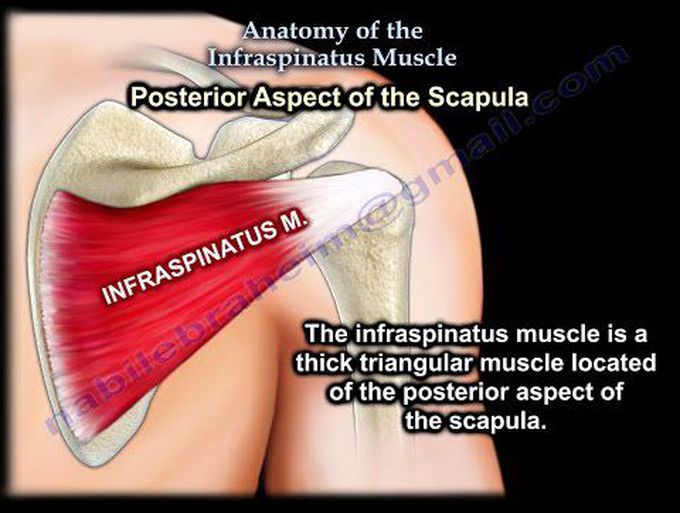
The infraspinatus muscle is a thick triangular muscle located at the posterior aspect of the scapula. The infraspinatus tendon inserts into the middle facet of the greater tubercle of the humerus. The infraspinatus is one of four muscles of the rotator cuff: 1-Teres minor 2-Infraspinatus 3-Supraspinatus 4-Subscapularis The infraspinatus is the primary external rotator of the arm and it also helps to stabilize the humerus. Innervation: the suprascapular nerve gives branches to the supraspinatus muscle and branches to the infraspinatus muscle. The suprascapular nerve passes under the transverse scapular ligament at the suprascapular notch. Compression of the suprascapular nerve at the suprascapular notch will result in atrophy of both the supraspinatus and infraspinatus muscles. Compression of the nerve distal to the spinoglenoid notch will lead to isolated weakness of the infraspinatus muscle. The phenomenon is seen with overhead athletes. It is usually associated with SLAP or posterior labral tears. Entrapment of the nerve at the spinoglenoid notch usually occurs due to a ganglion cyst. Important facts: rotator cuff tears occur in about 80% of patient over 60 years of age with shoulder dislocation. Posterior approach of the scapula: it utilizes the plane between the infraspinatus and the teres minor muscles. This plane is usually safe. Avoid going distal to the teres minor muscle due to the location of the axillary nerve. This approach to the posterior scapular is usually used for glenoid fractures and osteotomy. Hills- Sachs lesion Anterior dislocation causes defect on the posterior aspect of the humeral head. A large defect more than 25% of the humeral head is called an Engaging Hills- Sachs lesion. An operation called Remplissage is done to fill the Engaging Hills- Sachs lesion. Remplissage it is an infraspinatus and capsular transfer. Also check for possible Bankart lesion. Atrophy of the infraspinatus muscle is another problem. Massive tears of the rotator cuff that are greater than 5 cm usually involves multiple tendons. MRI will show massive cuff tear with retraction at the level of the glenoid with atrophy of the muscle and fatty infiltration. Muscle atrophy is usually seen on the sagittal image. Options for repair: •If there is a repairable posterior rotator cuff tear, the latissimus dorsi is transferred to the greater tuberosity. •Must have an intact subscapularis tendon and it is usually done in younger patients with massive tear of the rotator cuff. 2- Reverse shoulder arthroplasty: •Usually done in patients older than 70 years of age who have cuff arthropathy and anterosuperior escape (humeral head migrates proximally). •Must have a functional deltoid muscle (axillary nerve is unaffected) •If the axillary nerve is affected along with a massive rotator cuff tear, shoulder fusion is considered.
What is Rheumatoid Arthritis? | Johns Hopkins RheumatologyAnkylosing Spondylitis | HLA-B27, Pathophysiology, Signs & Symptoms, Diagnosis, TreatmentWhat is scoliosis?Osteosarcoma - Pathology, Symptoms, Diagnosis, TreatmentExternal nose bones
