


Renal disease
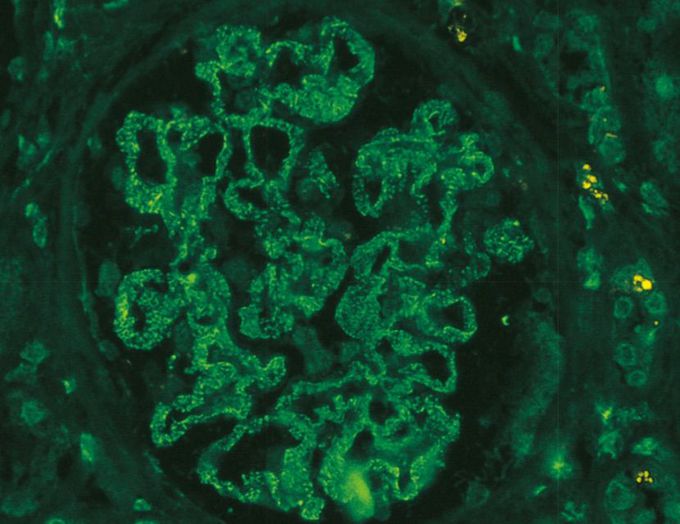
A 44-year-old man with increasing malaise for the past month now is bothered by increasing swelling in the hands and legs. On physical examination, there is generalized edema. He is afebrile, and his blood pressure is 140/90 mm Hg. Urinalysis shows a pH of 6.5; specific gravity 1.017; 4+ proteinuria; and no blood, glucose, or ketones. Microscopic examination of the urine shows no casts or RBCs and 2 WBCs per high-power field. The 24-hour urine protein level is 4.2 g. A renal biopsy specimen is obtained, and immunofluorescence staining with antibody to the C3 component of complement produces the pattern shown in the figure. Which of the following underlying disease processes is most likely to be present in this man? A. Chronic hepatitis B virus infection B. HIV infection C. Multiple myeloma D. Recurrent urinary tract infection E. Nephrolithiasis —�—�—�—�—�—�— . “spike and dome” appearance ->membranous nephropathy may be associated with HBV/HCV, solid tumors, SLE, or drugs One of the most common causes of nephrotic syndrome in adults is membranous nephropathy, caused by immune complex deposition, shown in the figure as extensive granular deposits with C3. About 75% of cases are idiopathic and due to autoantibodies reacting against podocyte antigens; but some cases follow infections (e.g., hepatitis, malaria), or are associated with causes such as malignancies or autoimmune diseases. In some cases of AIDS, a nephropathy resembling focal segmental glomerulosclerosis occurs. Multiple myeloma can be complicated by systemic amyloidosis, which can involve the kidney. Recurrent urinary tract infections are typically caused by bacterial organisms and can cause chronic pyelonephritis. Nephrolithiasis may lead to interstitial nephritis, but it does not cause glomerular injury.

I was diagnosed as a Hepatitis B carrier in 2015, with early signs of liver fibrosis. At first, antiviral medications helped control the virus but over time, resistance developed, and the effectiveness faded. I began to lose hope. In 2021, I discovered NaturePath Herbal Clinic despite my skepticism, I decided to give their herbal treatment a try.To my surprise, after just six months, my blood tests came back negative for the virus.It was nothing short of life-changing.I never expected such incredible results from a natural treatment. But it not only cleared the virus it restored my hope, my health, and my peace of mind.If you or someone you know is battling Hepatitis B, I truly encourage you to explore the natural healing path offered by NaturePath Herbal Clinic. It gave me a second chance and it might do the same for you.www.naturepathherbalclinic.com info@naturepathherbalclinic.com
