


Iris Abscess
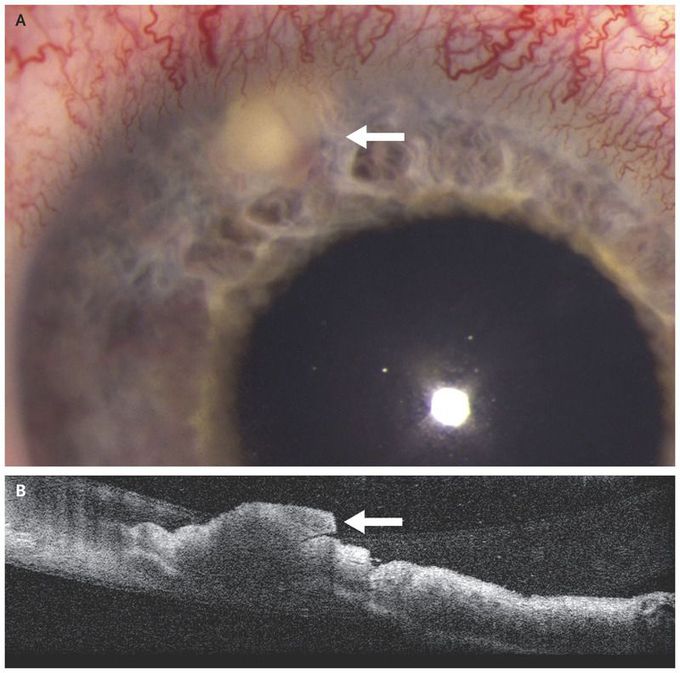
A 25-year-old woman presented to the retina clinic with progressive pain and redness in her right eye. She had a history of intravenous drug use, and 1 week before presentation she had received a diagnosis of methicillin-sensitive Staphylococcus aureus bacteremia and endocarditis, for which she was receiving intravenous antibiotic treatment. The visual acuity was 20/100 in the right eye and 20/20 in the left eye. Examination of the right eye revealed an iris lesion 3 mm in diameter (Panel A, arrow), a moderate number of inflammatory cells in the anterior chamber, dilated iris and limbal vessels, and the absence of vitreous cells. Anterior-segment optical coherence tomography confirmed the presence of an iris nodule (Panel B, arrow). Diagnostic anterior-chamber and vitreous samples yielded no organisms on Gram’s stain and no growth on culture. The clinical findings were consistent with a diagnosis of an iris abscess caused by bacteremia. In a patient with bacteremia, pathogens can spread to vascularized tissues, including the uvea and retina. Intraocular infections can be endogenous, resulting from hematologic spread of a systemic infection, or exogenous, resulting from trauma or intraocular procedures. In addition to 6 weeks of intravenous antibiotic therapy, the patient received intraocular vancomycin and ceftazidime, as well as moxifloxacin, prednisolone acetate, and cyclopentolate eyedrops. At follow-up 2 weeks after diagnosis, the iris nodule and inflammation had resolved, and a small iris scar was present.